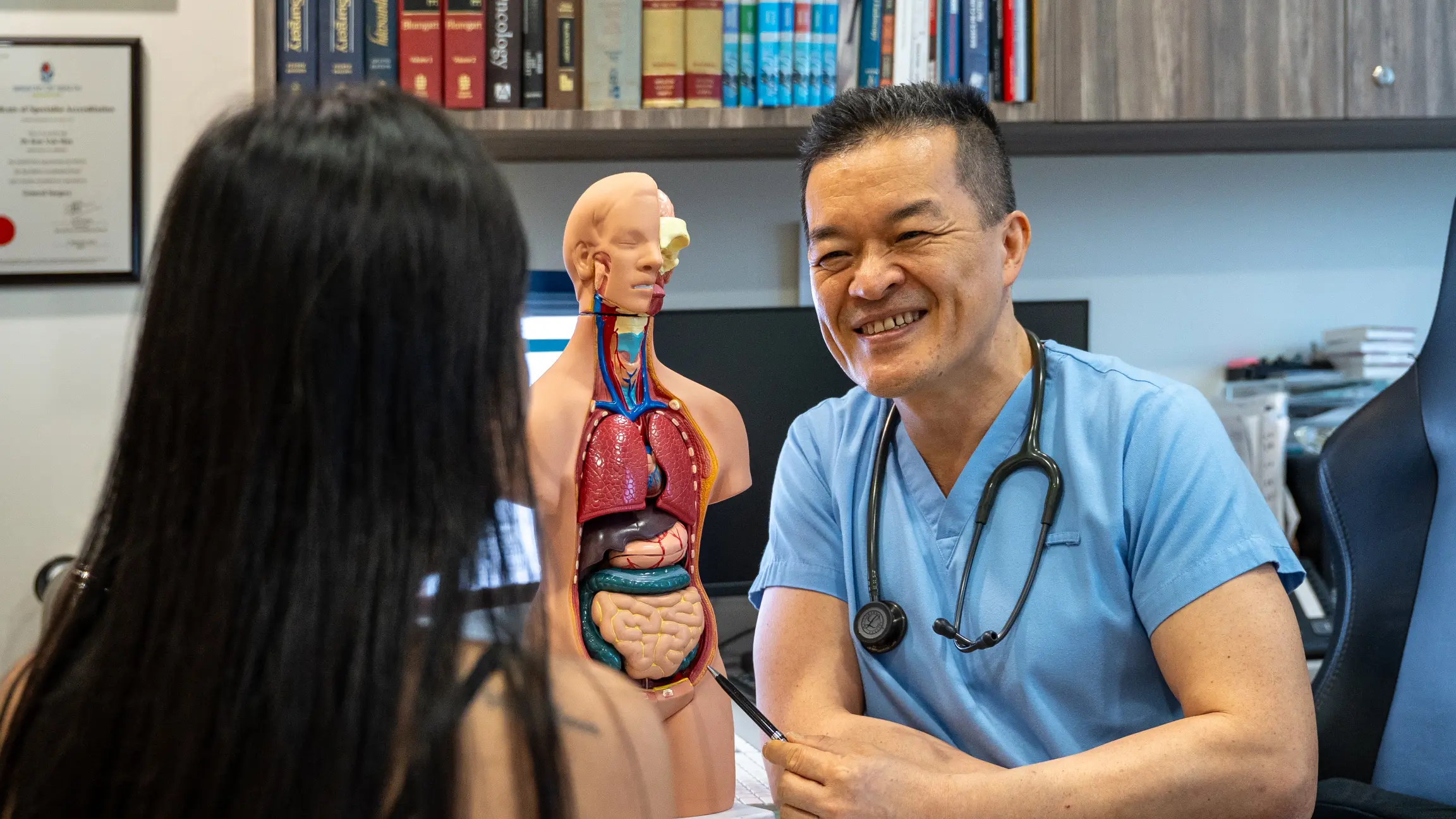







A flexible tube with a camera is passed through the mouth to directly visualise the oesophageal lining and collect tissue biopsies. Quick, performed under light sedation.
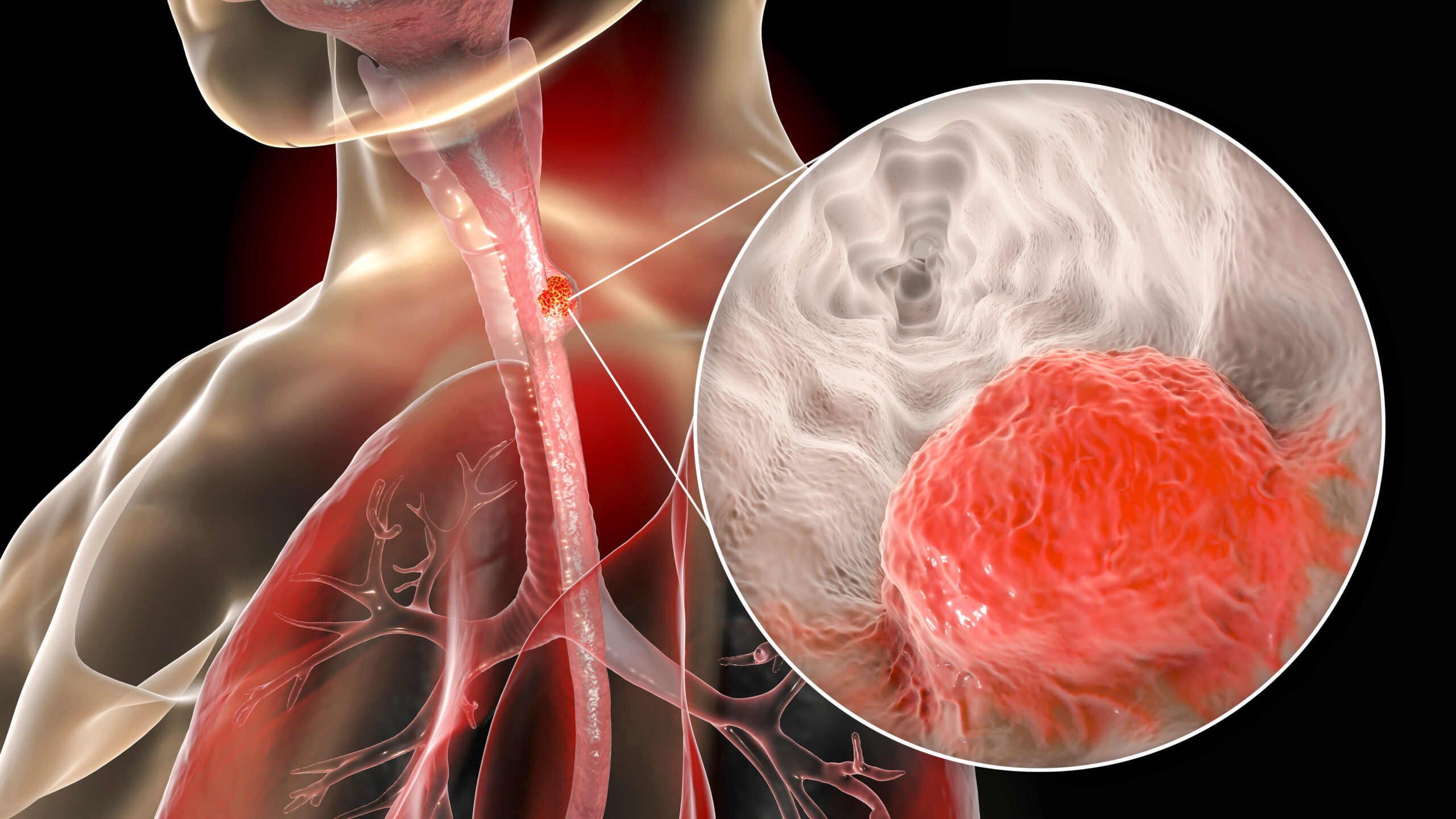
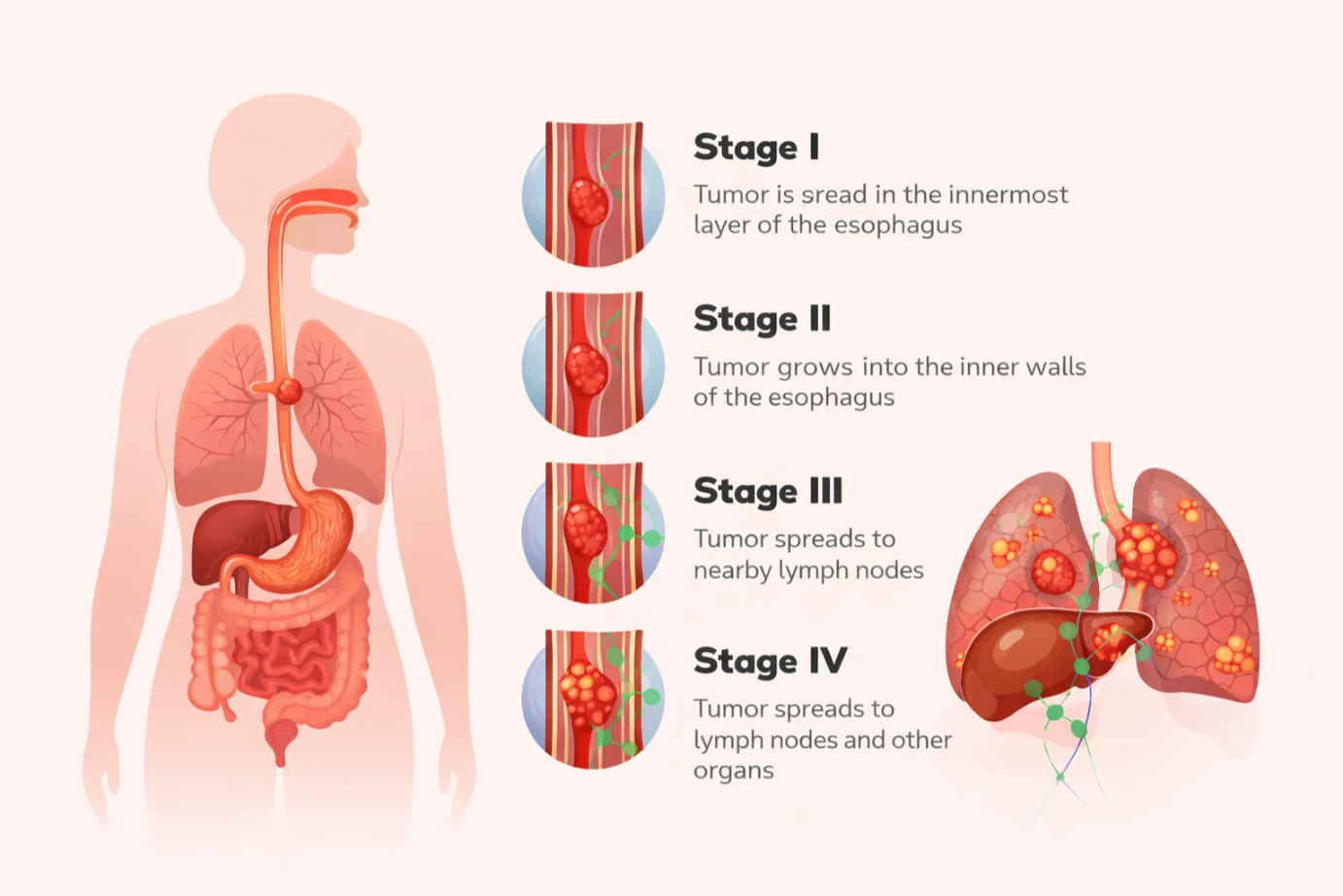
Advanced imaging provides detailed pictures of the oesophagus and surrounding structures to determine cancer stage and guide treatment planning.
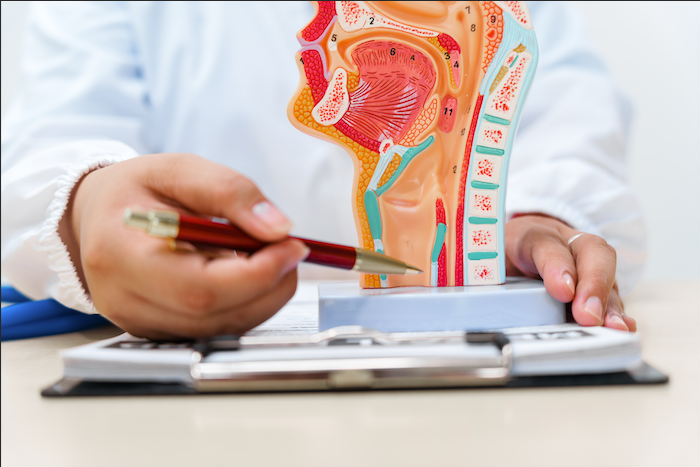
Tissue samples from the endoscopy are analysed by pathologists to confirm cancer presence, determine type (squamous cell or adenocarcinoma), and assess aggressiveness.